
Texaggie7nine said:Where are you getting that?Quote:
What percentage of the healthy population under 50 requires hospitalization. Under 1%? We can handle that.
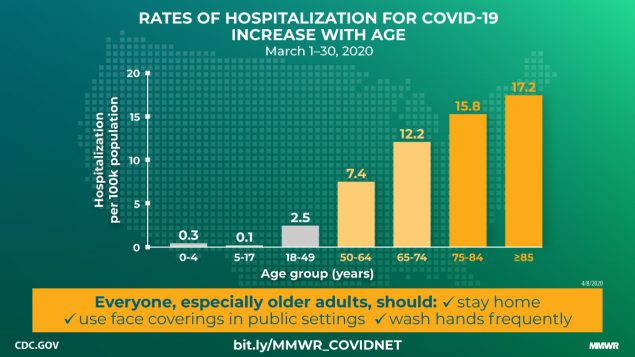
It's 2.9 per 100k for everybody under 50 according to this chart from the CDC
Texaggie7nine said:Where are you getting that?Quote:
What percentage of the healthy population under 50 requires hospitalization. Under 1%? We can handle that.
I saw you corrected. Yeah, 2.9% and 2.9 per 100k are 2 completely different things.PJYoung said:Texaggie7nine said:Where are you getting that?Quote:
What percentage of the healthy population under 50 requires hospitalization. Under 1%? We can handle that.
It's 2.9 per 100k for everybody under 50 according to this chart from the CDC
PJYoung said:Texaggie7nine said:Where are you getting that?Quote:
What percentage of the healthy population under 50 requires hospitalization. Under 1%? We can handle that.
It's 2.9 per 100k for everybody under 50 according to this chart from the CDC
The chart is not narrowed down to people who are infected. It is per 100k people in our entire population.Squadron7 said:PJYoung said:Texaggie7nine said:Where are you getting that?Quote:
What percentage of the healthy population under 50 requires hospitalization. Under 1%? We can handle that.
It's 2.9 per 100k for everybody under 50 according to this chart from the CDC
So less than 1 in 5 over 85 years old required hospitalization?
Texaggie7nine said:The chart is not narrowed down to people who are infected. It is per 100k people in our entire population.Squadron7 said:PJYoung said:Texaggie7nine said:Where are you getting that?Quote:
What percentage of the healthy population under 50 requires hospitalization. Under 1%? We can handle that.
It's 2.9 per 100k for everybody under 50 according to this chart from the CDC
So less than 1 in 5 over 85 years old required hospitalization?
Quote:
several ways to go with comorbidities, sex, age combos.
So assuming around 75% get infected we are looking at roughly 6.5 million hospitalizations and 1.65 million in the ICU. What was the total hospital capacity and ICU capacity? Those numbers sound like they would overwhelm hospitals if they occurred over a very short time window.k2aggie07 said:
The metric has been 80/15/5... 80% mild, 20% hospitalized... 15% severe, 5% ICU.
But that is of observed symptomatic cases. So, Assume 7:1 observed to not. That means if you had 80 / 20 before, it's really 780 / 20, making your total hospitalization rate around 2.5%.
This table in Imperial is probably pretty accurate, except.. make everything under 30-39 something like 0.1 to 0.5% with what we know now...
https://www.imperial.ac.uk/media/imperial-college/medicine/sph/ide/gida-fellowships/Imperial-College-COVID19-NPI-modelling-16-03-2020.pdf
HouAggie2007 said:Knucklesammich said:
The ambassador to the most powerful country on Earth, speaking officially for his government is not advised on what he can and cannot say? When that country is taking a novel approach to handling the pandemic in their country?
Ok, you are right he just says what he wants and is totally unsupervised.
We talking Trump or the sweede?
If true, this is kinda bigly big, isn't itplain_o_llama said:
Combining PFR with the Princess Diamond cruise ship IFR for ages above 70 we estimate the infection rates (IR) of regions in Italy, which peak in Lombardia at 23% (12%-41%, 95% c.l.), and for provinces in Bergamo at 67% (33%- 100%, 95% c.l.). This suggests that Bergamo may have reached herd immunity, and that the number of infected people greatly exceeds the number of positive tests, by a factor of 35 in Lombardia .
cone said:
just look at the NYC sero data
there's a total of 40000 hospitalizations in NYC so far and the sero study predicted 1.6 MM w/ antibodies
that's 2.5% across all ages
hospitalization rate under 50 is half the total rate per 100k people
so a 2.5% hospitalization rate across full cohort would indicate 1.25% for <50
that's not accounting for comorbidities
so even if you're thinking the NYC sero study is off, it's likely the upper bound for under 50 hospitalizations is ~2%
Quote:
Denmark and Norway are now beginning to ease their lockdowns, with children returning to school in the past 10 days, in smaller classes with markers to help keep them two meters apart. Salons and other businesses with one-to-one contact will reopen in Norway from Monday. Finland has extended its restrictions until May 13.

Quote:
Albert believes that Sweden's healthcare system is coping, as does Peter Lindgren, managing director at the Swedish Institute for Health Economics (IHE). Lindgren told CNN that the number of people treated in intensive care units over several weeks had been stable, "so in that aspect it has to be successful."
But he added: "What it failed at, I think, is that there has been disease transmitted into elderly care facilities. We have deaths occurring as a consequence of that."
Hallengren, the Swedish health minister, told CNN: "One of the main concerns now in Sweden is to strengthen the protection for those living in care homes for older people."
She said it was still "far too early to draw any firm conclusions as to the effectiveness of the measures taken in Sweden."

HotardAg07 said:
cone said:
just look at the NYC sero data
there's a total of 40000 hospitalizations in NYC so far and the sero study predicted 1.6 MM w/ antibodies
that's 2.5% across all ages
hospitalization rate under 50 is half the total rate per 100k people
so a 2.5% hospitalization rate across full cohort would indicate 1.25% for <50
that's not accounting for comorbidities
so even if you're thinking the NYC sero study is off, it's likely the upper bound for under 50 hospitalizations is ~2%
Isn't it too early to say?Squadron7 said:HotardAg07 said:
Isn't this to be expected, though? The question can't be answered until we get to a point where we can measure the area under the curve. And, again, if hospitals are not currently overwhelmed in Sweden then will still can't say that theirs is not the better way to herd immunity.
Quote:
If we had their per capita death total, we would have 20,000 more dead people.
Because the virus has spread though more of the population already? Front loaded deaths versus steady stream of deaths with a long tail?Squadron7 said:Quote:
If we had their per capita death total, we would have 20,000 more dead people.
I think this has been asked before...but why would per capita death totals be so different before any hospitals are overrun there? For that matter....why are they so different between states here?
Probably. What is Sweden's estimated IFR again?The_Fox said:Because the virus has spread though more of the population already? Front loaded deaths versus steady stream of deaths with a long tail?Squadron7 said:Quote:
If we had their per capita death total, we would have 20,000 more dead people.
I think this has been asked before...but why would per capita death totals be so different before any hospitals are overrun there? For that matter....why are they so different between states here?
I can only speculate.Squadron7 said:Quote:
If we had their per capita death total, we would have 20,000 more dead people.
I think this has been asked before...but why would per capita death totals be so different before any hospitals are overrun there? For that matter....why are they so different between states here?
Squadron7 said:Probably. What is Sweden's estimated IFR again?The_Fox said:Because the virus has spread though more of the population already? Front loaded deaths versus steady stream of deaths with a long tail?Squadron7 said:Quote:
If we had their per capita death total, we would have 20,000 more dead people.
I think this has been asked before...but why would per capita death totals be so different before any hospitals are overrun there? For that matter....why are they so different between states here?

NASAg03 said:
I don't believe Sweden is emphasizing testing the public at large, which skews the IFR.

