And some more...
As is usually the case, despite what my grade school teacher friends like to tell people, Wikipedia is a treasure trove of information once you follow references...
https://www.nature.com/articles/nm1267Again, rodent models. But it appears that a well-cited article from 2005 described a good deal of mechanism related to SARS spike protein, lung injury, and renin-angiotensin system. Of note:
- ACE2 is the major binding point for SARS spike protein. (This is well staged in all media today.)
- Binding of the spike protein to ACE2 significantly
down-regulates ACE2 expression.
- Binding of the spike protein to ACE2 in models of acute lung injury significantly worsened lung injury, but not in ACE2 KO mice (ie, the worsening was specific to spike protein-ACE2 binding)...but wait for it...
-
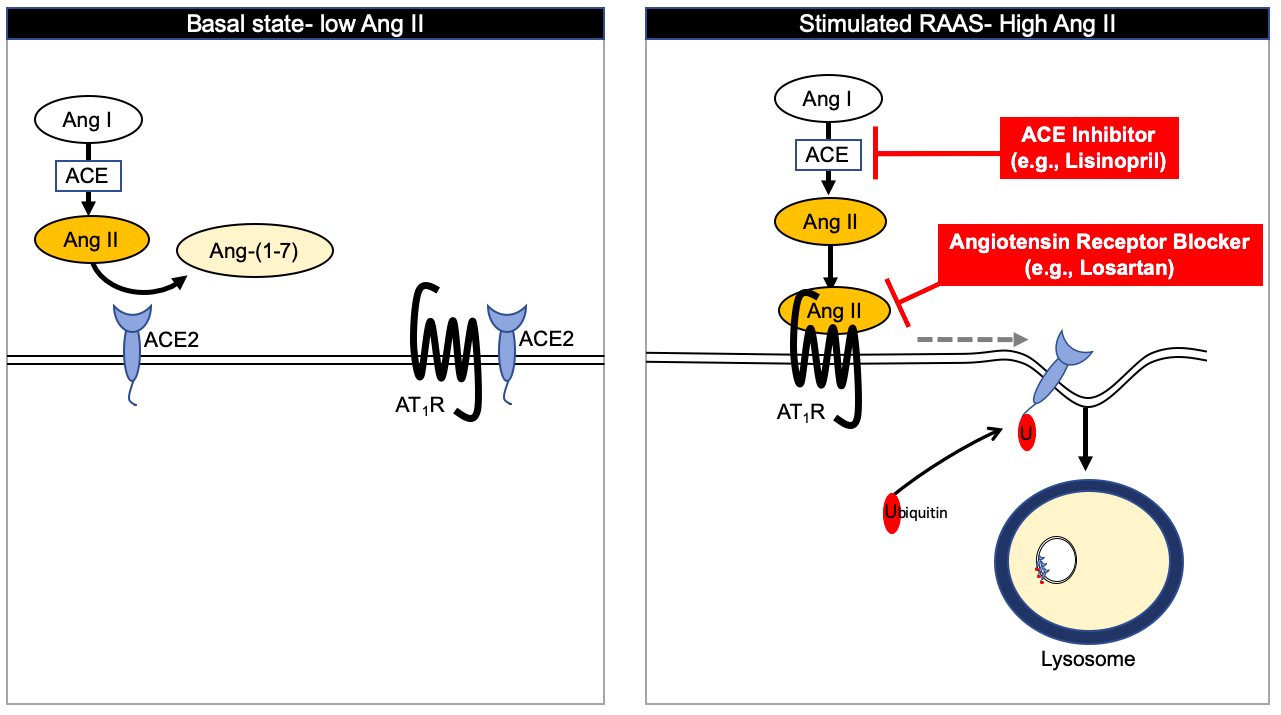
the Spike protein induced lung injury, as well as pulmonary edema, were attenuated with treatment of AT1R inhibitor (Losartan at 15mg/kg [probably not a good human dose])
So, Infection happens by binding to ACE2, the reduces ACE2 expression, thereby destabilizing renin-angiotensin system and making lung injury more severe.
If true, something that might increase ACE2 expression might have some protective effect with respect to severity of lung injury, a major part of what is reported to be killing people.
Now for some blind speculation....Many of the experiments in that paper were conducted with a recombinant spike protein to make sure that this binding was the source of what was studied. Therefore, destabilization of renin-angiotensin was caused only by the binding to the surface receptor (not some other action by the virus).
Several of the vaccine development projects I've read about are based on the spike protein. In fact, Moderna's mRNA vaccine, as I understand it, is intended to deliver mRNA to encode the CoV spike protein for the host cell to reproduce and then make antibodies against.
If the spike protein itself can cause so much damage, what's the chance that vaccines that present spike protein as the antigen might cause lung injury themselves. Hopefully muted if the vaccine is not inhaled, but ***** Hopefully also muted by giving as a finite dose that doesn't also replicate itself.
**** like this is why they need to be tested in safety trials and not distributed in mass as soon as a lab says they have one.