Article Discussing Diet, Cholesterol and Lipoproteins
I'm kind of a newb to the cholesterol game but trying to learn more since my LDL levels were a little high on my last doctor visit. My current understanding is that LDL broadly is a lipoprotein that carries cholesterol (among other things) around in the blood stream, LDL-c is the amount of cholesterol in a given LDL and LDL-p is the number of LDL particles in the blood stream.
But the following example in the article above is confusing me:
Is this a bad example or am I missing something? Shouldn't LDL-p be the number of buckets, not the number of balls?
I'm kind of a newb to the cholesterol game but trying to learn more since my LDL levels were a little high on my last doctor visit. My current understanding is that LDL broadly is a lipoprotein that carries cholesterol (among other things) around in the blood stream, LDL-c is the amount of cholesterol in a given LDL and LDL-p is the number of LDL particles in the blood stream.
But the following example in the article above is confusing me:
Quote:
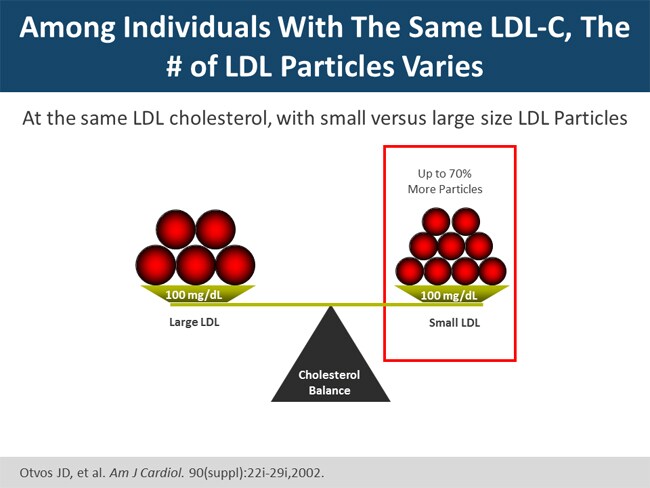
In order to understand how LDL-c, LDL size and LDL-p are interrelated, imagine that you are going to fill a bucket with golf balls and tennis balls.
The bucket is the total amount of cholesterol contained within LDL (LDL-c). The golf balls are small LDLs, while the tennis balls are Large LDLs.
The total number of balls is the LDL particle number.
You can fill the bucket with either tennis balls, or golf balls. The bucket will be just as full, but if you use golf balls the number of balls in the bucket will be much greater.
Is this a bad example or am I missing something? Shouldn't LDL-p be the number of buckets, not the number of balls?